- Viewed - 2160
- Printed - 0
- Emailed - 1
- PDF Downloaded - 41
A CASE REPORT OF CONGENITAL CORNEAL OPACITY
Year : 2021 | Volume : 1 | Issue : 0 | Page :
MJWI.2022/94
Dr. Prajakta V. Bhailume , Dr. Mayuri R. Bakhade ,
Date of Web Publication 29-Mar-2022
Keywords
congenital corneal opacity, congenital rubella infection, congenital cytomegalovirus infection
A CASE REPORT OF CONGENITAL CORNEAL OPACITY
INTRODUCTION: Congenital corneal opacity refers to the opacification of cornea present at birth. It can occur as an isolated anomaly or with systemic association. It is a rare condition and is an important cause of corneal blindness. Prevalence of congenital corneal opacities is estimated to be around 3 in 100,000 newborns. Sensory visual deprivation due to opacification of cornea in the phase of visual development leads to sensory deprivation amblyopia. Management of congenial corneal opacity consists of early diagnosis and treatment. Penetrating keratoplasty is indicated for the corneal opacity.
CASE DETAILS: A 10 days old male child is brought by his parents to the ophthalmology OPD with complaints of whitish discolouration of cornea in right eye noted since birth.
Birth History: Second born male child, Full term normal vaginal delivery, delivery was uneventful, baby cried immediately after birth, no h/o NICU admission. Birth weight was 2.4 kg, h/o maternal infection during pregnancy.
Family history: H/o death of first born child due to cardiac anomaly at the age of 1 year. H/o polyhydramnios during 1st pregnancy.
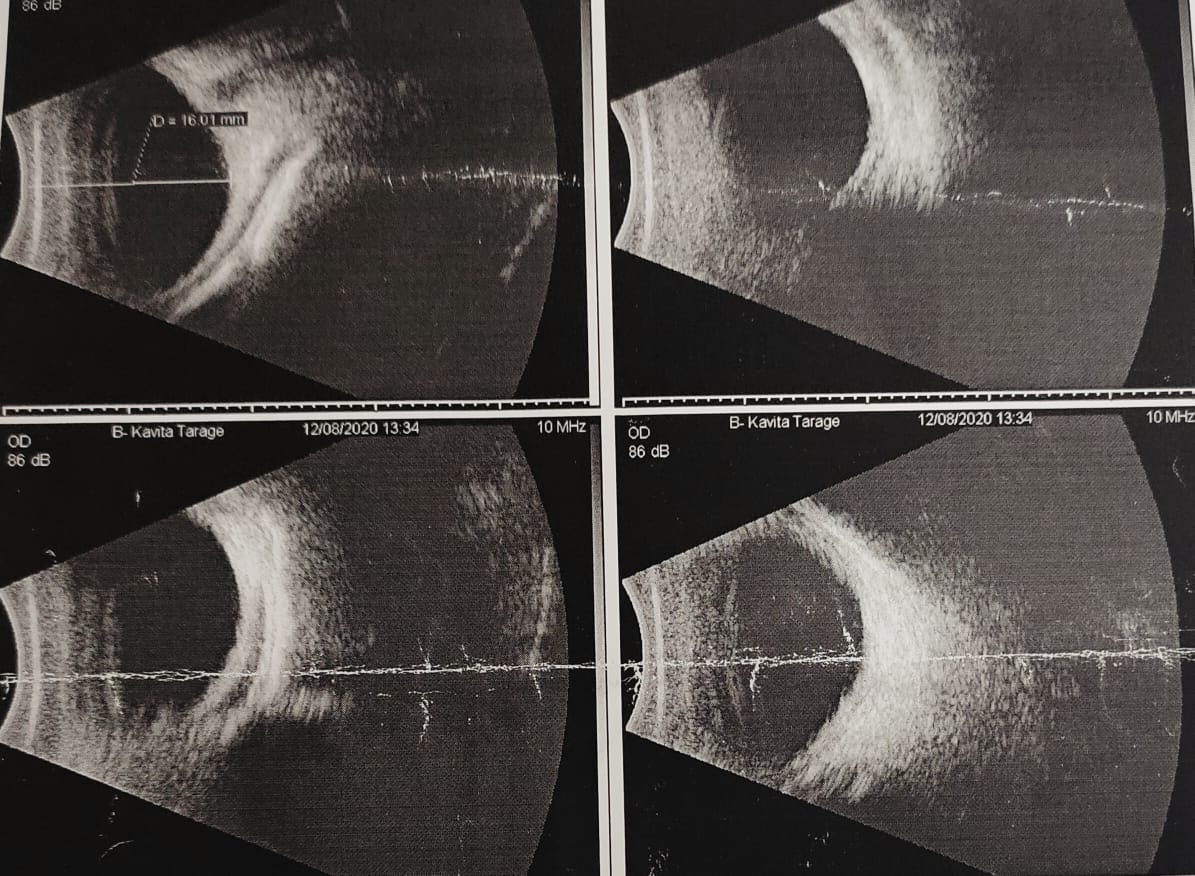
Ocular Examination:
[
[
SYSTEMIC EXAMINATION
CNS: NAD
CVS: Pan-systolic murmur
RS: AEBE
PA: Hepato-splenomegaly
- Paediatric referral for further evaluation
INVESTIGATIONS:
-TORCH TITRE
Rubella IgG titre: positive (85.2 IU/mL); Rubella IgM: negative (10 AU/ml)
CMV IgG titre: positive (156 U/mL); CMV IgM: negative (5 U/ml)
-CBC: WBC count: 10,000/cumm; RBC count: 4.69 milli/cumm;
platelets: 3 lakhs/cumm; Hb: 16.8 g/dl
-LFT: Direct bilirubin: 0.36 mg/dl; Indirect bilirubin: 7.54 mg/dl;
-USG Cranium: Normal
-USG Abdomen: hepatosplenomegaly
-Hearing evaluation: SNHL
-2D-ECHO: VSD
DIAGNOSIS
Right Eye Congenital Corneal Opacity secondary to Congenital Rubella and Cytomegalovirus infection
PLAN OF MANAGEMENT:
Penetrating Keratoplasty
DISCUSSION:
Congenital corneal opacity refers to the opacification of cornea present at birth. It can occur as an isolated anomaly or with systemic association. It is a rare condition and is an important cause of corneal blindness. Prevalence of congenital corneal opacities is estimated to be around 3 in 100,000 newborns. (1) Unilateral corneal opacities are generally isolated, while bilateral opacities are often associated with systemic conditions and a complete genetic workup is essential. (2) Sensory visual deprivation due to opacification of cornea in the phase of visual development leads to sensory deprivation amblyopia.
Differential diagnosis of congenital corneal opacities :( 3)
-Corneal dystrophies: - Congenital hereditary endothelial dystrophy
- Congenital hereditary stromal dystrophy
- Posterior polymorphous corneal dystrophy
-Peter’s anomaly
-Infections: - congenital rubella, herpes simplex, cytomegalovirus and bacterial
- Anterior segment dysgenesis: sclerocornea, anterior staphyloma
-Dermoid
-Trauma: forceps delivery trauma
-Metabolic disorders: mucopolysaccharidoses, cystinosis
-Congenital glaucoma
-Developmental anomaly of iridotrabecular system: Axenfeld-Reiger syndrome
Management of congenial corneal opacity consists of
-Early diagnosis and treatment. Penetrating keratoplasty is indicated for the corneal opacity.
-Treatment of concurrent ophthalmic and systemic conditions.
-Prevention of sensory deprivation amblyopia and visual impairment.
Treatment of congenital corneal opacity is often challenging and complicated because of reduced scleral rigidity and increased elasticity. This increases the risk of anterior displacement of lens-iris diaphragm and wound retraction with associated lens expulsion.
Early diagnosis of underlying aetiology and surgical intervention is essential to prevent sensory deprivation amblyopia. (4, 5)
CONCLUSION: Congenital Corneal opacities, though rare, pose a significant morbidity to a child’s visual function. Various genetic, developmental, infectious and metabolic conditions cause congenital corneal opacities. Early diagnosis of underlying aetiology and surgical intervention is essential to prevent sensory deprivation amblyopia. A detailed evaluation and timely intervention decrease the morbidity and mortality.
REFERENCES:
1) Bermejo E, Martinez-Frias ML. Congenital eye malformations: clinical epidemiological analysis of 1,124,654 consecutive births in Spain. Am J Med Genet. 1998; 75:497–504.
2) Bhandari R, Ferri S, Whittaker B, Liu M, Lazzaro DR. Peters anomaly: Review of the literature. Cornea 2011;30:939-44.
3) Rezende RA, Uchoa UB, Uchoa R, Rapuano CJ, Laibson PR, Cohen EJ. Congenital corneal opacities in a cornea referral practice. Cornea. 2004 Aug; 23(6):565–70.
4) Zaidman GW, Rabinowitz Y, Fortstot SL. Optical iridectomy for corneal opacities in Peter’s anomaly. J Cataract Refract Surg 1998;24:719-22.4.
5) Parmaley VC, Stonecipher KG, Rowsey JJ. Peters’ anomaly: A review of 26 penetrating keratoplasties in infants. Ophthalmic Surg 1993;24:31-5.
Source(s) of support: Nil
Presentation at a meeting:
Organisation: BJGMC and SGH, Pune
Place: Pune
Date: 23/04/2021
Conflicting Interest (If present, give more details):
Nil