- Viewed - 2229
- Printed - 15
- Emailed - 9
- PDF Downloaded - 231
Significance of C-Reactive Protein levels in children with Malaria in a tertiary care centre –a cross sectional study.
Year : 2022 | Volume : 1 | Issue : 0 | Page :
MJWI.2022/99
Dr.Ramya Srinivasa Rangan , Dr CT Deshmukh , Dr Jane JE David , Dr Smita Anil Divate ,
Date of Web Publication 17-Apr-2022
Keywords
C Reactive Protein,malaria
Abstract:
Background and objective:
To measure and compare the CRP levels among the various species of malaria, among simple and complicated malaria and to correlate CRP with the outcome.
Methods:
Cross sectional observational study of malaria positive children conducted over a period of 18 months.
Results:
Of the 67 children included in our study,39 weremale and 28 female children.Plasmodium Vivax was seen in 60 (89.6%) cases,mixed malaria (both P.Vivax and P.Falciparum) cases were 5 (7.5%) and Plasmodium Falciparum were two (3%) cases.In total 12 patients (17.9%) had normal CRP and 55 patients(82.1%) had high values.Out of 60 patients of P.Vivax ,50had high CRP (> 7mg/l ), both patients of P. Falciparum had high CRP and CRP values ranged from normal to high for thosewith mixed infection. There was no association foundbetween species of plasmodium and CRP values (p>0.05). Of the 53 patients with simple malaria, 43 patients (81%) hadhigh CRPwhileten had normal values.Complicatedmalaria, was seen in 14 patients with 12 (85%) patients having high CRP values. The association between the CRP levelsand the severity of malaria was not statistically significant (p> 0.05). The association between CRP and shorter duration of hospital stay, low platelet counts and high SGOT levels was found to be statistically significant.
Conclusion:Elevated CRP in a febrile child could also point towards malaria in a tropical country like India.CRP can be utilized as a biomarker in assessing the severity and outcome of malaria.
Key words:C Reactive Protein,complicated malaria,Low platelet counts, Plasmodium Vivax,simple malaria.
Introduction:
The 2020 estimates that from the year 2000 to 2019 the malaria cases have reduced by 73% in the WHO South-East Asia Region and in India it has reduced from about 20 million cases in 2000 to about 5.6 million in 2019. Malaria deaths have reduced steadily in WHO South-East Asia Region over the period 2000 to 2019 by 74%, yet India accounted for about 86% of all malaria deaths1.Fever of acute onset without a focus is a common diagnostic dilemma in children. Self-limiting viral infections (common cold) and uncomplicated bacterial infections (otitis media, pharyngitis) are the commonest causes of acute fever in children. Malaria usually presents with fever,headache, chills and other symptoms.However, malaria in children may not always manifest with the classical relapsing pattern of fever. The overlapping of malaria symptoms with other tropical diseases impairs diagnostic specificity, which can promote the random use of anti malarial drugs and compromise the care for patients with non-malarial fevers in endemic areas 2.
Over the years the peripheral smear has been the gold standard for diagnosis, but needs to be done frequently and can be negative in many patients. Rapid malarial antigen testing has been used in recent times with very good results. However, the rapid diagnostic tests remain positive for months after malarial infection and cannot be used for assessing the response.C Reactive Protein (CRP) is a simple and easily available testfirst discovered by Tillett and Francis in 1930 at the Rockefeller University3.CRP has been found to be useful in supportingdiagnosis, to assess response to therapy and for guiding treatment in casesof bacterial infections,inflammatory, immunological conditionsand connective tissue disorders. Studies have shown that CRP levels are elevated inparasitic infection like malaria and it is also associated with severity of malaria.Hence timely prediction of severity would help in early treatment of lifethreateningcomplications of complicated malaria.As CRP is a cost effective marker and readily available, this study was conducted forassessing whether CRP has a role in malaria infections in children, and whether it isassociated with the disease severity and outcome.
Objectives:
To measure and compare the CRP levels among the various species of malaria, to see the difference in CRP among simple and complicated malaria, to correlate CRP with the outcomeand to look for its value in prognosis of malaria.
Material and Methods
Children were recruited in this cross-sectional observational study over a period of 18 months from January 2017 to June 2018 in a Tertiary Care Centre. Ethics committee approval was taken from the Institutional Ethics Committee of our Institution. Children found to be malaria positive either by Peripheral smear or Rapid Diagnostic Kit (RDT)-MAT {Malaria Antigen Test} were included in the study.Children suffering from other co infections like dengue, leptospirosis etc. were excluded.Informed and free consent was obtained from the parents of the malaria positive childrenfor sending blood samples for CRP levels. CRP was measured using Immunoturbidimetric method. Normal CRP levels was taken as 0 to 6 mg/l and high CRP levelswas more than or equal to 7 mg/l.CRP levels were analysed and compared in different species of malaria, P. Vivax, P. Falciparum and mixed infection (both P. Vivax and P. Falciparum).CRP levels were compared in simple and complicated malaria.The correlation of CRP with respect to the outcome of the patient like the duration of the hospital stay,discharge or death was observed. Mean, Median and Standard deviation was used to study discrete variables. To compare the CRP levels between P. Vivax and P. Falciparum cases and also to compare it with other parameters,Pearson’s Correlation Coefficient /Chi Square test was used. Mann Whitney U test was used to compare the two groups of normal and high CRP levels versus other discrete variables.
Results:
We studied 67 children affected with malaria, the male: femaleratio was 1.39.Most of them were from5 to 10 years (38.8%) of age with a mean age of 5 years. Plasmodium Vivax infection was the major species encountered that is 60 cases (89.6%) followed by five (7.5%) cases of mixed infection and with only two cases (3%) of P. Falciparum malaria. As per the WHO definition, simple malaria was found in 53 children(79.1%)and complicated malaria seen in 14(20.9%) children.The mortality observed was 1.5%, with the death of one childwith complicated malaria.Among the discrete variables observed,clinical pallor was seen in 50 children (75%), of whom four presented with severe anemia (Hb < 5gm/dl).Hepatomegaly was seen in 15(22.4%) children, and 19 children (28.4%) had splenomegaly. The mean duration of hospital stay was three days, the mean hemoglobin values was 9.6 gm/dl and the mean platelet count was 1,30,000/mm3.
Normal CRP values was seen in 12 children (17.9%) and high CRP values was seen in 55 children (82.1%) with 33 (60 %) of them having high CRP valuesof more than 50 mg/l. The mean CRP among all children was 65 mg/l[Table 1].The association between the CRP levels and the meanage or gender of the children wasfound to be statistically insignificant (p>0.05). In relation to the malaria species ,50 children with P.Vivax infection and twochildren with P. Falciparum infection had high CRP values more than 7mg/l. The children who had mixed infection (both P.Vivax and P.Falciparum), had varying CRP values ranging from normal to high. There was no association found between the species of plasmodium and CRP values (p> 0.05).Though the mean CRP levels was raised insimple as well as complicated malaria with aslightly higher level in complicated, it was not found to be statistically significant.The association between CRP levels with the duration of hospital stay, low platelet counts and SGOT levels was found to be statistically significant(p value <0.05).Higher CRP levels were found when the hospital stay was of shorter duration,there was a lower platelet count, and when the SGOT levels were higher. However, the association of CRP with other parameters like organomegaly (hepatomegaly and splenomegaly),serum sodium levels, SGPT levels, blood sugar and mean hemoglobin levels was not found to be statistically significant [Table 2].The association between CRP and outcome of the disease was not significant as there was only one death with a mortality of 1.5% in a child with complicated falciparum malaria and the remaining children recovered and were discharged.
Discussion
In areas with a high prevalence of malaria,high degree of clinical suspicion is required for prompt diagnosis and timely and life saving interventions. Inflammatory markers like CRP may help in such situations. High CRP values of 7 to 50 mg/l was seen in 22 (32.8 %) children in our study and very high CRP values of more than 50 mg/l was seen in 33(49.3%)children.Normal CRP levels of 0 to 6 mg/l was seen in only 12 (17.9%) children. Dipthi et al4 (n=50) in her study has also shown a similar finding with 3 (6%) patients with normal CRP, and 29 (58 %)patients with CRP values between 7 to 50 mg/l and 18 (36%)patients with very high CRP values > 50 mg/l.On the contrary Naik et al5 showed that the group of healthy malaria negative children from Zambia also had a mean CRP of 5.2 µg/ml (high) due to high endemicity in African areas. Also Eriksson et al6 in their study showed that even in the control group (malaria negative) (n=258), the median CRP was 39 mg/l (range5 to 480 mg/l). They concluded that CRP could not be used to diagnose or differentiate malaria and other non malaria febrile illness.
In our study,60 (89.6%) cases had P.Vivax infection, followed by five (7.5%) cases of mixed infection and two (3%) cases of P.Falciparum. Over the past few years the malaria trends have been fluctuating with a significant drop in the number of cases especially during our study period andthe severity of cases and infection with P.Falciparum also had dropped, with more of P.Vivax cases being seen. A similar pattern of species distribution was seen in a study by Dipthi et al4 (n=50) showing 30(60%) P.Vivax,16(32%) mixed and 4(8%) cases of P.Falciparum infection. In our study, there was no significant association between CRP and species of plasmodium. Eriksson et al6 also showed that there was no association between species of plasmodium and CRP levels of malaria infected patients. But there are many studies which showed that CRP values were higher in P.Falciparum compared to P.Vivax infection4,7,8[Table 3].
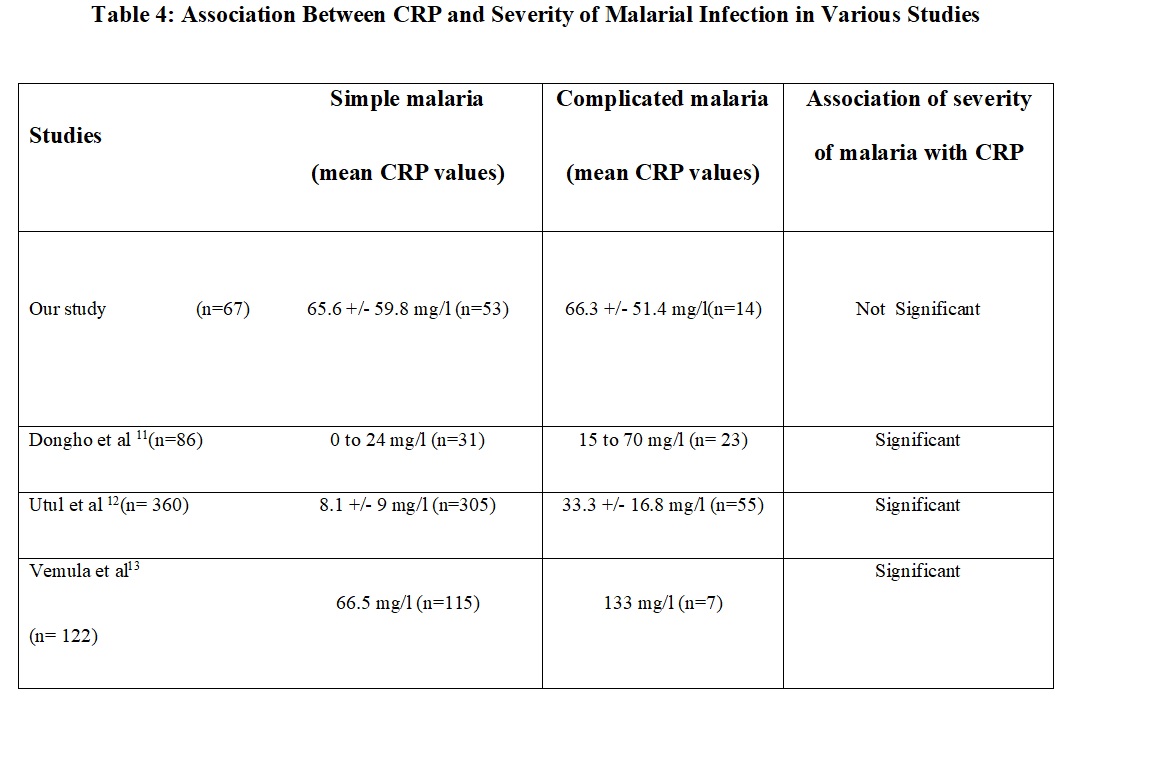
In our study, simple malaria was seen in 53 (79.1%) childrenand 14 (20.9%) had complicated malaria.We found the mean CRP levels was raised in simple as well as complicated malaria though it was slightly higher in complicated malaria,it was not found to be statistically significant. However, Donell et al9showed that CRP was raised in simple malaria (203 µg/ml) more than in severe malaria patients (47µg/ml) and the reason proposed was that CRP has a protective role in severe malaria and its levels are lower in severe malaria due to failure to control the inflammatory response to infection that may contribute to the progression to severe disease and death10,11,12 [Table 4].
The mean duration of hospital stay in our study was three days. There was a statistically significant association with highCRP levels and short duration of hospital stay which can be attributed to the fact that the CRP is high in the initial phase of illness (CRP plays a protective role against fighting the malarial infection and the cytokines released during fever stimulate the release of CRP) and then gradually the CRP levels declines as the fever subsides and during recovery phase of illness.This is in contrast to the study conducted by Pelkonen et al13 and Chhatriwala et al7 who showed that longer the length of hospital stay, higher is the CRP values.
We found a statistically significant association between low platelets(< 1,50,000 /mm 3) and high CRP levels.Thrombocytopenia was observed in 50 of our children.The CRP was found to be high in 45children with thrombocytopenia and normal in 5 children.This was similar to a study by Agrawal et al 8 where there was inverse correlation between CRP and platelet counts in P.Falciparum patients (correlation coefficient = -0.46).Chhatriwala et al7also showed that there was a statistically significant negative correlation between platelet count in P.Falciparum infection (correlation coefficient = -0.51).
In our study, the mean SGOT values of all children were higher in those with high CRP values and the association was statistically significant. Both Agrawal et al10 and Chhatriwala et al 9 in their study showed that there was a significant positive correlation between CRP concentration and serum concentrations of SGOT and SGPT in P.Falciparum infection but not in P.Vivax infection.
In our study, 98.5 % children were discharged with a mortalityof 1.5% (One case of severe falciparum malaria). The study conducted by Dipthi et al 4 had no mortality whereas the mortality in Donell et al9 was 0.02% (cases in the group of severe malaria cases). We had no case of cerebral malaria. A study by Pelkonen et al13 showed12% (n=28) cases of cerebral malaria.
Strengths of the study :Enrollment of malaria cases was considered throughout the year (not only in the monsoon season).
Limitation of the study: The sample size was small. A large sample size is needed to prove the beneficial role of CRP in a common infection like malaria.Most of the cases were of P.Vivax malaria compared to very few P.Falciparum cases hence the CRP values could not be correlated with the severity of P.Falciparummalaria.CRP was measured on admission only and serial measurement of CRP was not done which could have helped in proving CRP as a prognostic indicator while assessing the severity of malaria.CRP levels could not be correlated with the outcome in malarial infection as complicated malaria cases were few and mortality was minimum.
Conclusion
CRP levels may also be elevated in parasitic infections like malaria. Elevated CRP in a febrile child could also point towards malarial infection in a tropical country like India. CRP levels are higher in children with malarial infection who have low platelet counts, shorter duration of hospital stay and high SGOT levels.CRP being a cost effective marker and readily available,itcan be utilized as a biomarker in assessing the severity and outcome of malaria cases.
References :
Table 1 : Mean Values of CRP among Children with Malaria
[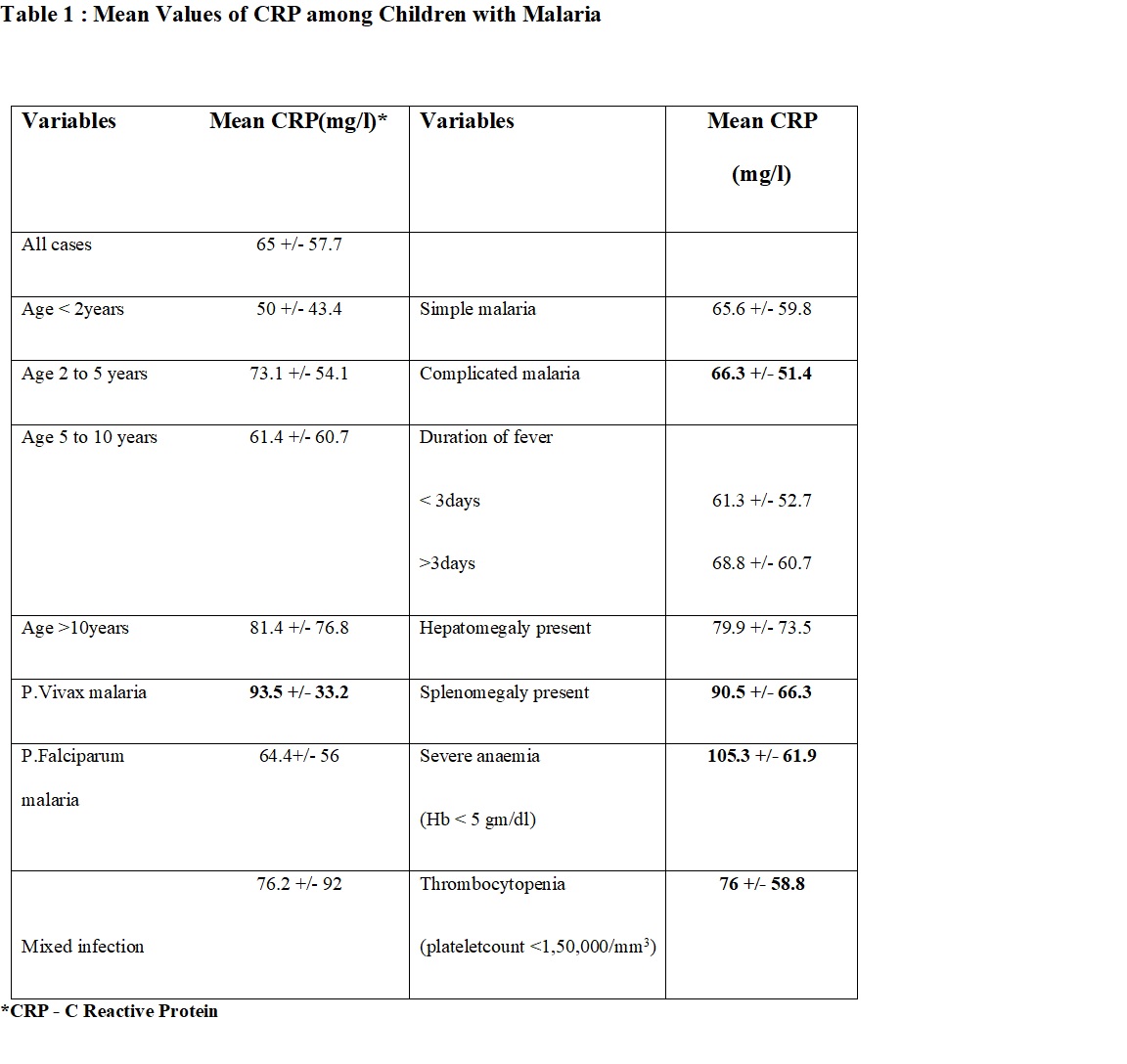
*CRP - C Reactive Protein
Table 2: Comparison of Clinical and Laboratory Parameters of Children with Malaria among the CRP* Groups.
[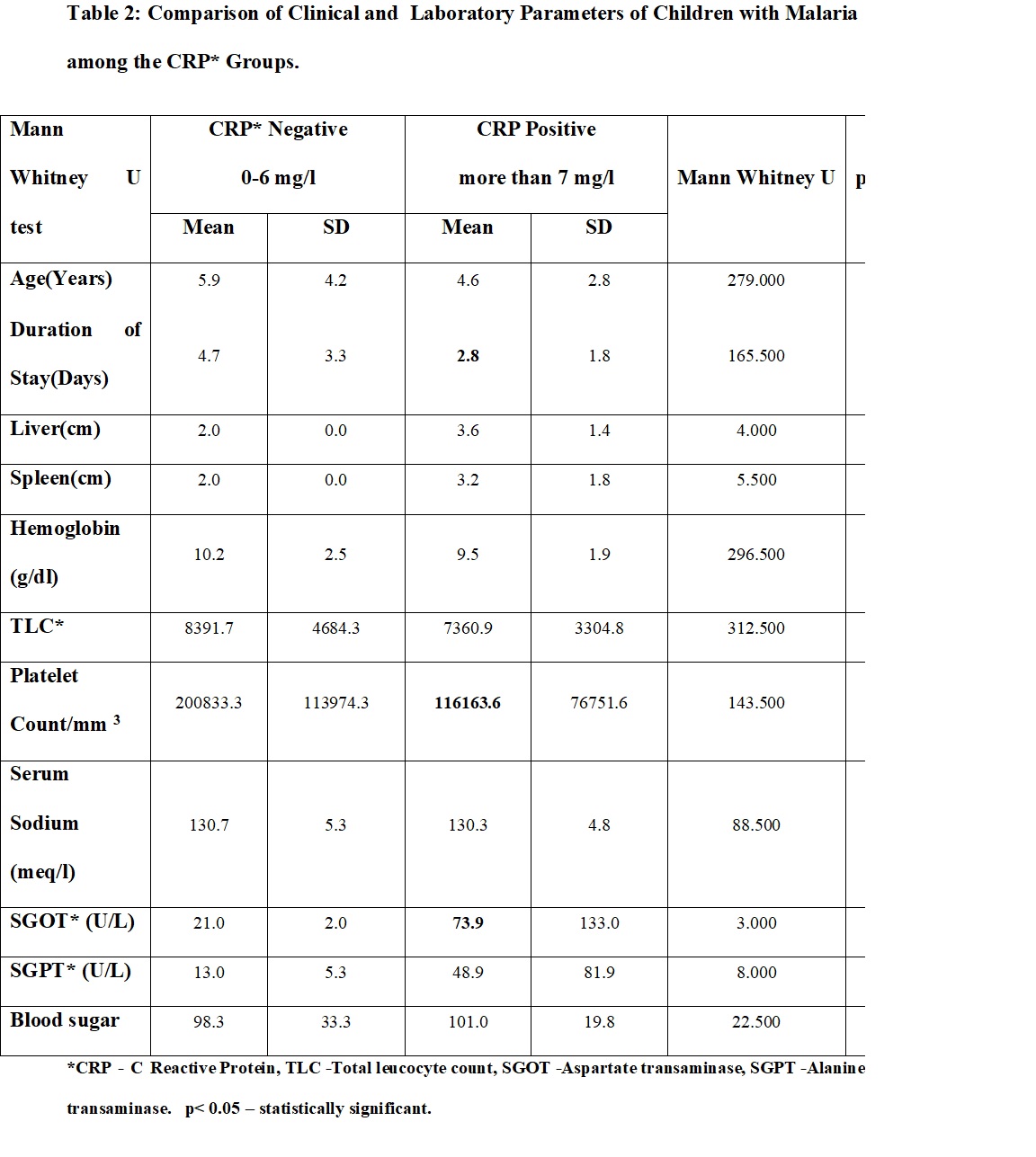
*CRP - C Reactive Protein, TLC-Total leucocyte count, SGOT-Aspartate transaminase, SGPT-Alanine transaminase. p< 0.05 – statistically significant.
Table 3: Mean CRP Values in Various Studies with Relation to Plasmodium Species.
[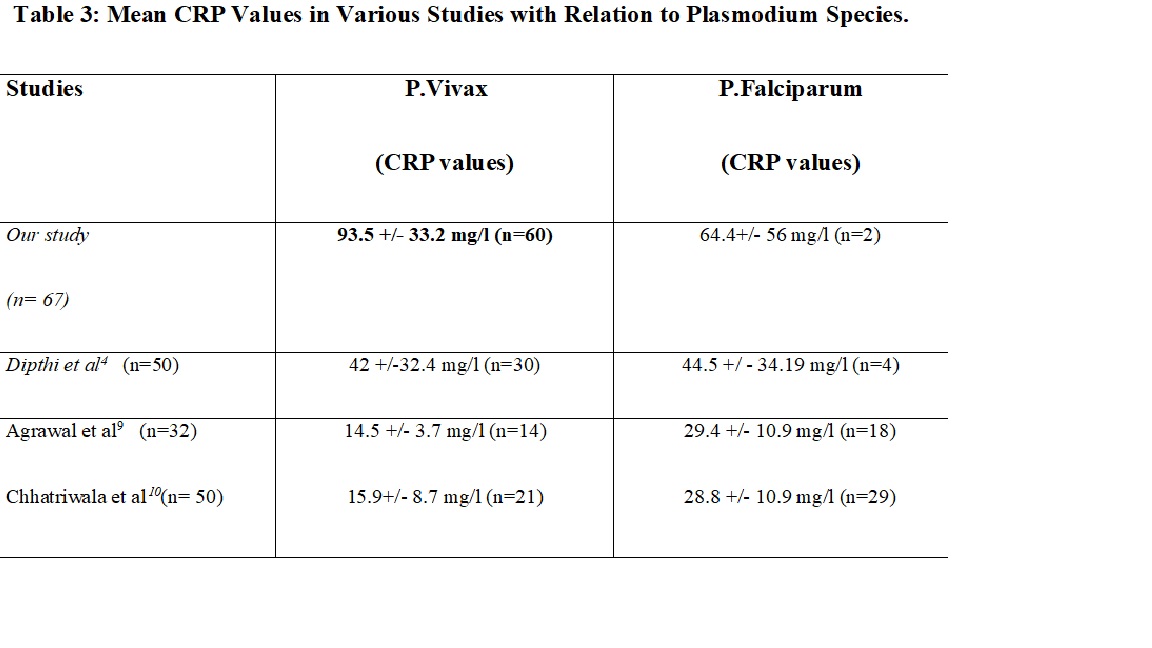
Table 4: Association Between CRP and Severity of Malarial Infection in Various Studies
[